
+918042752699

Currently it only shows your basic business info. Start adding relevant business details such as description, images and products or services to gain your customers attention by using Boost 360 android app / iOS App / web portal.
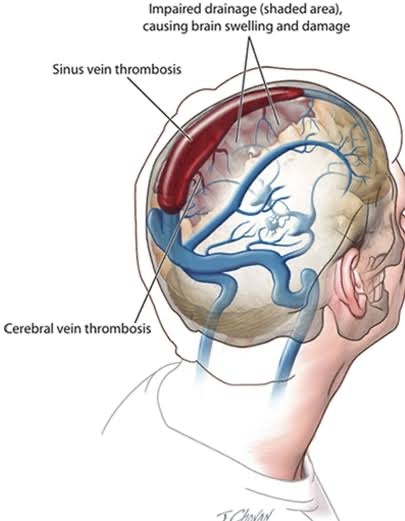
Below is a *1000-word, professionally written web-article* on **Cerebral Venous Thrombosis (CVT)**, tailored for a **neurointervention / clinical audience**, suitable for a medical website or patient-referral platform. It covers pathophysiology, diagnosis, imaging, interventional treatments, and outcomes. --- # **Cerebral Venous Thrombosis (CVT): A Comprehensive Neurointervention Perspective** **Cerebral Venous Thrombosis (CVT)** is a rare but potentially devastating cerebrovascular disorder in which blood clots form within the dural venous sinuses or the cerebral veins, leading to impaired venous drainage, intracranial hypertension, and ischemic or hemorrhagic brain injury. Though accounting for only 0.5%–1% of all strokes, CVT affects a **younger population** and is seen more frequently in **women**, especially those with hormonal risk factors. Early recognition and prompt management are critical—delays can lead to significant morbidity or mortality. Neurointervention plays an increasingly important role in selected patients, particularly those who fail medical therapy. This article reviews CVT from pathophysiology to advanced treatment, with a focus on interventional strategies that improve outcomes. --- ## **1. Pathophysiology and Risk Factors** The cerebral venous system comprises cortical veins and dural sinuses (e.g., superior sagittal, transverse, sigmoid sinuses). Venous thrombosis disrupts normal outflow, causing: * **Venous congestion** * Elevated intracranial pressure (ICP) * Reduced cerebral perfusion * Vasogenic and cytotoxic edema * Parenchymal hemorrhage ### **Key Risk Factors** CVT is multifactorial; common associations include: * **Hypercoagulable states** • Inherited thrombophilia (Factor V Leiden, prothrombin gene mutation) • Antiphospholipid syndrome • Elevated homocysteine * **Hormonal influences** • Pregnancy and postpartum period • Oral contraceptives / hormone replacement therapy * **Systemic conditions** • Malignancy • Infection (e.g., mastoiditis, sinusitis) • Autoimmune disease (e.g., lupus) * **Medical interventions and trauma** • Central venous catheters • Head injury --- ## **2. Clinical Presentation** CVT presentation is highly variable. Common symptoms include: * **Headache**: Nearly universal; may be gradual or acute * **Focal neurologic deficits**: Weakness, sensory change * **Seizures**: Often generalized * **Visual symptoms**: Due to papilledema * **Altered consciousness**: In severe cases Because symptoms mimic other neurologic conditions, CVT can be misdiagnosed unless specifically suspected. --- ## **3. Diagnostic Evaluation** ### **Neurologic Examination** Assessment focuses on: * Signs of raised ICP * Focal deficits * Fundoscopy for papilledema ### **Laboratory Workup** * Complete blood count * Coagulation profile * Prothrombotic panels (when indicated) ### **Neuroimaging** Timely brain imaging is crucial. #### **Noncontrast CT (NCCT)** * May show hyperdense clot (“cord sign”) * Can detect hemorrhage or edema #### **CT Venography (CTV)** * Rapid assessment of venous system * Excellent detection of sinus occlusion #### **MRI / MR Venography (MRV)** * Most sensitive modality * Shows absence of flow, direct clot visualization * Identifies parenchymal changes #### **Digital Subtraction Angiography (DSA)** * Gold standard when diagnosis is unclear * Facilitates **interventional planning** --- ## **4. Standard Medical Management** ### **Anticoagulation** Even in the presence of hemorrhage, **anticoagulation** is first-line therapy: * **Low molecular weight heparin (LMWH)** acutely * Transition to **Vitamin K antagonists** or direct oral anticoagulants (DOACs) Goals: * Prevent clot extension * Facilitate recanalization * Reduce risk of new thrombosis ### **Adjunct Therapies** * **Analgesia** for headache * **Antiepileptic drugs** for seizures * **ICP management** (e.g., mannitol, hyperventilation, head elevation) * Treat underlying cause (infection control, hormonal adjustment) --- ## **5. When to Consider Neurointervention** While anticoagulation benefits most patients, **20–30% do not respond adequately**. Indications for endovascular intervention include: * **Neurologic deterioration despite anticoagulation** * **Extensive cerebral venous occlusion** * **Severe intracranial hypertension** * **Large hemorrhagic lesions threatening herniation** * **Contraindication to systemic anticoagulation** --- ## **6. Endovascular Techniques in CVT** Neurointerventional approaches aim to **mechanically disrupt the clot** and **restore venous outflow**. ### **Mechanical Thrombectomy** Uses stent retrievers and aspiration catheters to: * Physically remove clot from the sinus * Rapidly restore flow Key features: * High efficacy in revascularization * Reduced thrombus burden * Can be combined with other methods ### **Chemical Thrombolysis** Delivered locally via microcatheters into occluded sinuses: * Tissue plasminogen activator (tPA) infusion * Often used in conjunction with mechanical techniques Localized thrombolysis reduces systemic bleeding risks. ### **Balloon Angioplasty and Stenting** Considered when: * Underlying stenosis persists after clot removal * Flow restoration is incomplete Stents provide structural support to maintain sinus patency. --- ## **7. Procedural Outcomes and Safety** Endovascular therapy has shown: * Improved **recanalization rates** * Reduced **clinical deterioration** * Favorable functional outcomes in selected patients Complications are possible but rare: * Hemorrhage * Vessel injury * Contrast reactions Patient selection and operator experience critically influence safety. --- ## **8. Post-Intervention Care and Rehabilitation** Post-procedural care includes: * Continued anticoagulation * ICP monitoring * Neurologic observation * Physiotherapy and occupational therapy Long-term outcomes depend on: * Extent of initial injury * Timeliness of diagnosis and treatment * Control of underlying risk factors --- ## **9. Prognosis and Long-Term Management** CVT historically carried high mortality, but with modern care: * **Functional recovery rates exceed 80%** * Recanalization is common * Recurrence is low with appropriate anticoagulation Long-term considerations: * Duration of anticoagulation tailored to cause * Lifelong anticoagulation for persistent prothrombotic disorders * Regular imaging follow-up in complex cases --- ## **10. Future Directions in CVT Management** Emerging research areas include: * **Predictive biomarkers** for risk stratification * **Advanced imaging** for thrombus characterization * **Robotic and AI-assisted neurointervention** * Clinical trials comparing endovascular strategies with standard care As understanding deepens, individualized therapy will continue to improve outcomes. --- ## **Conclusion** Cerebral Venous Thrombosis is a complex but treatable cerebrovascular disease. The cornerstone of management remains early diagnosis and anticoagulation. However, neurointervention is a powerful tool in refractory or severe cases, offering direct thrombus removal and rapid flow restoration. With evolving technology and multidisciplinary care, many patients with CVT can achieve excellent functional recovery.
